|
Return to Articles Main Page
The ankle sprain is one of the most common sports-related injuries, with lateral (outside) ankle injuries occurring most often. Adequate understanding of the anatomy, mechanism, diagnosis and treatment of these injuries is essential for doctors who treat ankle sprains.
Anatomy
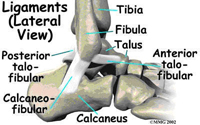
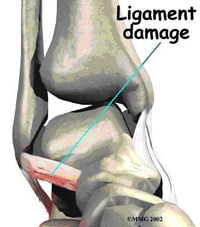
The lateral ankle ligaments are the anterior talofibular (ATFL), calcaneofibular (CFL), and posterior talofibular ligaments (PTFL).The ATFL is the most commonly injured lateral ankle ligament. When theses ligaments are disrupted, the ATFL usually tears first, followed by the CFL, and lastly, the PTFL. |
|
Mechanism of Injury
|
The history given by the injured person is a valuable tool in the evaluation of ankle injuries. The person may recall hearing a “pop” or “snap.” He/she may also be able to relate the position of the foot and the motion that occurred during the injury. This recollection may give insight as to the mechanism of injury and therefore indicate the anatomic structures likely to have been injured – which may help in distinguishing lateral ankle sprains from “high” ankle sprains.
History may provide evidence of ankle instability. People may relate a history of multiple ankle sprains in the past as well as a recurrent problem with their ankle “giving out.” The ability to bear weight following an ankle sprain should be ascertained. An inability to bear weight suggests a more severe injury. |
|
Physical Exam
The examination begins with inspection. The degree and location of swelling, discoloration and any gross deformity should be noted. The physical examination may be difficult to perform soon after the injury, due to pain. There is commonly swelling over the outside of the ankle. There may be tenderness to palpation of one or more of the ligaments.
|
The anterior drawer test is a test that the doctor may perform to determine the stability of the anterior talofibular ligament. The lower portion of the leg is held firmly while the heel is cupped and drawn forward. If the talus (ankle bone) is drawn 4mm or greater than the uninjured side, there is likely ATFL damage. (1)
The talar tilt test may evaluate the ankle ligament stability. For this test the lower leg is held firmly while the foot is tilted inwards. This procedure needs to be done under local anesthesia. If the talar tilt is 5 to 10 degrees greater than the uninjured side, ligament damage is likely. (1) The exam should also be performed in a manner that will evaluate the differential diagnoses listed below. Without this thorough evaluation, a significant injury may be missed, causing the person to have long-term pain that is not responsive to typical ankle injury treatment. |

|
Radiography
X-rays are commonly obtained to rule out fracture, particularly if there is an inability to bear weight. Ankle sprains in children warrant radiographic evaluation to rule out fracture of the growth plate.
Diagnosis
Once diagnosed, lateral ankle sprains are classified. Grade I injuries involve a stretch of the ligament without tear or instability. There is mild pain or swelling and the ability to bear weight is preserved. Grade II injuries involve a partial tear of the ligament with mild instability. There is moderate pain, swelling, and ecchymosis with some difficulty bearing weight. Grade III injuries consist of complete tear of the ligament with severe instability. There is severe pain, swelling, ecchymosis and the inability to bear weight.
It is not uncommon that additional foot problems occur along with the more severe ankle sprains. Some of these include: fifth metatarsal base fractures, fractures of the front portion of the heel bone and fractures of the top of the ankle bone.
Treatment
Treatment of acute ankle sprains should focus on rehabilitation with the goal of preventing chronic instability. Initial therapy of acute ankle sprains should reduce pain and inflammation. This is done with RICE therapy (rest, ice, compression, elevation). Anti-inflammatory medications may be used to reduce pain while narcotic medications are rarely necessary.
Grade I injuries are usually treated with RICE, bracing followed by taping, protected weight bearing and rehabilitation. Treatment is usually three weeks.
Grade II injuries are treated in the same manner with the exception that the patient may need to progress from partial to full weight bearing. Treatment is usually six weeks.
Grade III injuries are treated in a similar manner although there is an initial period of non-weight bearing. There is a progression to partial followed by full weight bearing. Treatment is usually six to eight weeks. Competitive athletes with Grade III injuries may undergo surgical repair. The general population can be treated with conservative care with rehabilitation. If there is continued pain or instability, surgery may be performed at a later date.
When possible, we encourage patients to begin range of motion exercises as soon as possible after the injury. Isotonic strengthening exercises with elastic tubing in plantar flexion, dorsiflexion, inversion and eversion may be started as early as possible. We also encourage patients to be weight bearing as soon as they are able. Only the most severe injuries need cast immobilization.
The degree and extent of rehabilitation is dependent upon the level of function that returns to the patient. Pain and swelling may be used as a guide. Home exercises may be given initially, but those injuries not responding after one to two weeks may need a formal physical therapy referral.
There are certainly varied opinions and controversy regarding the methods and regimens used in the treatment of the ankle sprain as well its rehabilitation. Many clinicians have their own preferences, however the goals of treatment are clear: relief of pain and inflammation, preservation of strength and a return to activity with stability.
Return to Articles Main Page
Our Services | Referring Physicians | About Us | Frequently Asked Questions | Blog | Articles
Surgical Animations | Links | News & Press | Photo Gallery
Contact Us | Home | Legal Notice | Privacy Statement | Site Map
Copyright © Buffalo Medical Group P.C. / Podiatry Affiliates
Website Design, Maintenance and Hosting by Catalyst Marketing / Worry Free Websites |
